The Evolution of Treatment Options for Diabetic Macular Edema
UWF™ retinal imaging with optomap®. This has been confirmed by UWF fluorescein angiography (FA).
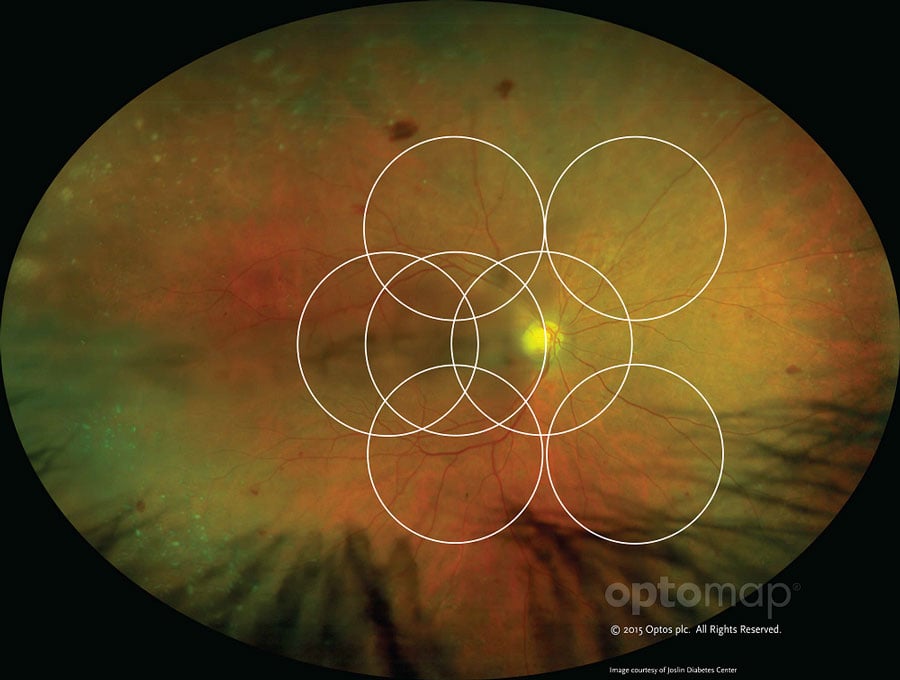
optomap captures 82% or 200 degrees of the retina, with DME and DR often presenting outside the ETDRS
Rapid visualization of the peripheral retina with UWF color and FA imaging (often without a mydriatic agent) allows more pathology to be found at an earlier onset. Peripheral ischemia is determined with confirmatory FA which documents peripheral neovascularization, nonperfusion, and late peripheral vascular leakage. Earlier diagnosis allows earlier treatment. Thus, UWF retinal imaging is now employed regularly in clinical trials to assess the benefits of treatment protocols. The treatments utilized and compared in the majority of trials include panretinal photocoagulation (PRP) in proliferative disease, vascular endothelial growth factor (VEGF) inhibitor therapy, and combination therapy incorporating laser treatment guided by UWF color and FA imaging.
Treatment Options
Of course, the treatment of any diabetic complication involves the control of the diabetes itself via blood sugar management, blood pressure control, and lipid management.
Diabetic retinopathy (DR) and DME are now treated earlier with the knowledge of peripheral disease, and the conventional severity scoring methods (i.e. 4-2-1) are not as effective as they once were. A standard evaluation may see elements of DR, but with the advent of UWF color and FA imaging our treatment approaches are changing. It is now much more clearly understood that peripheral disease begets DME, and it can take on an acute or chronic appearance.
Acute DME
We are aware that the hyperglycemia of DM causes disease of the retinal capillaries, which in turn causes hypoxia of the retina, producing the acute release of VEGF. Clinical trials have shown that when a VEGF inhibitor (VEGFI) is used to treat an ischemic retina and followed by PRP, a remarkable resolution of DME can occur. Furthermore, delivering two injections of VEGFI a month apart can reduce the effects of PRP-induced VEGF secretion. Should DME remain persistent, a re-evaluation with UWF FA can determine what area of the retina is still ischemic, and repeat targeted PRP can be performed.
Chronic DME
Chronic DME has a significant inflammatory component and can result in irreversible tissue damage. The tissue damage causes the release of numerous cytokines, such as interleukin-6, interleukin-8 and MCP1. These inflammatory mediators need to be controlled, and in addition to VEGF inhibition and PRP, steroid treatment must be employed.
Iluvien (fluocinolone acetonide intravitreal implant) 0.19mg (Alimera Sciences), a recently approved injectable implant, is a new option for treatment of DME. Iluvien consists of tiny, cylindrical tube containing fluocinolone acetonide that is implanted in the back of the eye via a 25-gauge needle and releases submicrogram levels of the drug for 36 months. Adverse effects are increased IOP and cataract development.
As demonstrated in RISE and RIDE trials, there was less improvement in vision when the affected retina with chronic DME was treated. Resultantly, the need for early treatment is critical. These studies clearly documented that when DME was treated within two years, there was an improved response due to the lack of irreversible damage.
Forward Progress
The use of UWF and optomap technology have a number of preventative benefits. As an office procedure, it is much more efficient and produces valuable information. Visualizing the peripheral retina identifies earlier changes and can prevent a devastating loss of vision. Conservation of time during evaluation from elimination of dilation and indirect ophthalmoscopy may permit more direct patient contact, discussion about treatment options, identification of barriers to compliance, and collaboration with other providers to address concerns in management of the patient’s disease.
For more information on UWF and optomap, please contact us.