UWF Retinal Imaging Enables Effective Ocular Telehealth Programs
The need to increase the rate and accessibility of ocular health screenings is significant. For example, of the 415 million adults worldwide who are afflicted with diabetes, 45 percent are undiagnosed. A large percentage of these undiagnosed individuals will develop diabetic retinopathy (DR) and DME diabetic macular edema (DME). Also important is the diagnosis of other conditions, many of which are found in aging populations, including age-related macular edema (AMD), branch retinal vein occlusion, glaucoma, and cataracts.
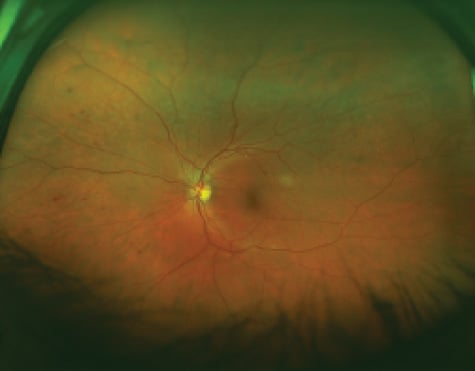
optomap image demonstrating predominantly peripheral diabetic lesions.
One way to widen the availability of ocular health screenings is through telehealth and telemedicine programs. These initiatives are growing worldwide as stakeholders in the health community take advantage of advances in medical and communications technology. One such innovation with particular utility in ocular telehealth is ultra-widefield (UWF™) retinal imaging, which offers an effective, rapid, and easy-to-use means bringing state-of-the-art diagnostics to underserved populations. This technology, developed by Optos, has been deployed in a variety of telehealth settings.
About Ultra-widefield Retinal Imaging
UWF retinal imaging is performed by a specially designed scanning laser ophthalmoscope (SLO) that generates a high-resolution digital image covering 200° (or about 82 percent) of the retina. By comparison, conventional 7 standard field (7SF) ETDRS photographs produce a relatively narrow view (45° or less) of the center-portion of the retina.
The SLO simultaneously scans the retina using two low-power lasers (red and green) that enable high-resolution, color imaging of retinal substructures. The resulting UWF digital image – the optomap – is produced in a single non-contact capture. Along with UWF color imaging, the technology supports UWF fluorescein angiography (FA), UWF fundus autofluorescence (FAF), and UWF indocyanine green chorioangiography (ICG).
UWF Retinal Imaging and Ocular Telehealth
UWF retinal imaging technology is uniquely suited for telehealth applications. Because all optomap images are digital, they can be transmitted to specialists, appended to EHRs (electronic health records), and used in patient education and follow-up. Compared to DR screening methods as such nonmydriatic fundus photography, UWF retinal imaging has demonstrated lower rates of ungradable images, faster evaluation times and more comprehensive assessments of DR severity.
Preliminary Results from an Ocular Telehealth Study
In this study, the authors examined the results of a pilot program in which patients were screened at four primary care clinics in southwest Missouri. optomap images were combined with the patient’s EHR and reviewed off-site by a board certified ophthalmologist. Recommendations on follow-up care were sent back to the primary care clinic using the EHR.
During the first 90 days of the program, 340 optomap images were reviewed and 55 patients were identified as having significant pathologies. They included 26 patients with DR, including 5 with proliferative diabetic retinopathy. Other conditions uncovered included branch retinal vein occlusion, age-related macular edema, cataract, asymmetrical cupping, and in one case, a nevus later diagnosed as melanoma. Normal primary care screening would never have captured these pathologies.
A Large-Scale Ocular Telehealth Program
A second, larger study reports on the on the relative effectiveness of UWF retinal imaging compared to NMFP (nonmydriatic fundus photography). The work was undertaken by a long-established telehealth program specifically intended to screen for DR and DME. This program has been in operation since 1998 and follows a strict evaluation protocol combined with an ongoing quality assurance plan that checks and re-evaluates about 10 percent of primary patient evaluations.
The study looked at results from 3,803 patients, of whom 1,633 were imaged with NMFP (producing three 45° fields) and the balance were scanned with UWF imaging (producing 100° and 200° fields). Both sets of subjects were statistically equivalent in regard to age, sex, diabetes duration and insulin use. The study found:
— Poor quality images that couldn’t be graded for DR totaled 2.9 percent of those scanned using UWF imaging versus 9.9 percent for those screened with NFMP.
— DR was identified in 38.4 percent of those screened with UWF imaging versus 33.8 percent of those screened with NFMP.
—Vision threatening DR was identified in 14.5 percent of those screened with UWF imaging versus 11.9 percent of those screened with NFMP.
—Follow-up studies looked at peripheral retinal changes outside the fields used by the evaluation protocols. Had these findings from the much wider UWF images been incorporated into the evaluation, the study’s authors estimated that 9 percent of the eyes would have been assigned a more severe level of DR.
The study also found that median evaluation time for NFMP images was 12.8 minutes per patient versus 9.2 minutes for UWF imaging – a 28 percent reduction.
Perhaps the most important outcomes of this study were how UWF retinal imaging (1) reduces ungradable images and (2) provides more comprehensive diagnostic results. In particular, better quality images significantly increased the impact and effectiveness of this ocular telehealth program.
The use of UWF retinal imaging in ocular telehealth programs will continue to expand in both primary care settings, as well as targeted screening initiatives. In both cases, the results will be more effective, comprehensive screening and improved health outcomes for patients who otherwise might never have been diagnosed and treated.

For more information:
Tauber, Shachar, Ocular Telehealth: A Wider View of the Need and the Opportunity in Ophthalmology, Retina Today, May-June 2015.
Silva PS, Cavallerano JD, Tolls D, et al. Potential efficacy benefits of nonmydriatic ultrawide field retinal imaging in an ocular telehealth diabetic retinopathy program. Diabetes Care. 2014;37:50-55.